About Breast Cancer
Breast Cancer is the most common cancer among women in India. Every year around 1.5 to 2 lakh new women are being diagnosed with Breast Cancer.
According to GLOBOCAN 2012,” India is facing challenging situation due to 11.54% increases in incidence and 13.82% increase in mortality due to breast cancer.”
In Urban areas 1 in 22 women are likely to be affected by breast cancer. Upto 50% of these don’t survive within 5 years of the diagnosis, More than half of the cases are detected at advanced stage i.e. Stage III and above i.e. majority of women in India when they are diagnosed with Breast cancer, the cancer has already progressed to arm pit or it has involved the Breast skin or nipple. Out of the two women who are diagnosed with Breast cancer only one survives due to advanced stage of disease presentation. In western population more than 80 % women are being detected when the disease is limited to breast, not spread to armpit or any other site in the body and having a small volume i.e. less than 2cm tumor size i.e. Stage I/ II with a survival rate of more than 80%.
Figure
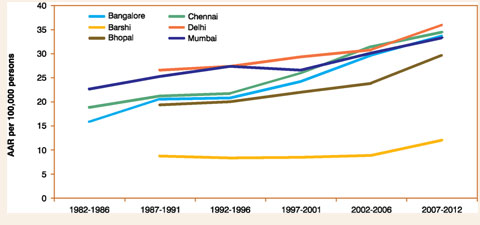
Inadequate screening and advanced stage of presentation are the main reasons for the rising death toll, along with limited medical facilities.
In the west majority cases present in Stage I & II, whereas in India 45.7% report in advanced stages(acc to Malviya etal, AP JCO2017). If cancer is detected at early stage the survival can reach upto 90% whereas when detected in advanced stage the survival falls down to less than 50%
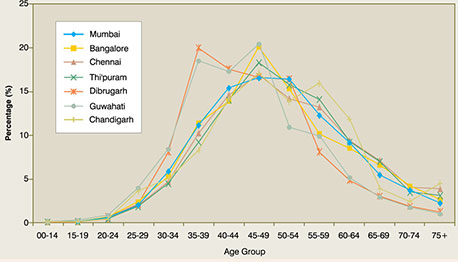
Lower age of Incidence (Malviya etal, AP JCO2017)
Another important aspect in Indiais the younger age of presentation of Breast Cancer 45 to 49 is the peak age of incidence of breast cancer across the country. In North East, this age has gone down to 35 years.
It is general thumb rule, younger the cancer, more aggressive it is, also Younger aged patients tends to have the more aggressive variety i.e. be triple negative cancer Younger age Breast Cancers below 40 are difficult to screen, the increased density of breasts in younger age group makes it difficult to be detected or seen in mammography, making mammography of limited utility. Breast Cancer in India is rising at a alarming pace, we definitely need to adjust our lifestyle, lead a healthy and stress free life; limit or control our habits. Timely Pregnancy in today’s times shall be 35 yrs or less, it definitely reduces the risk of Breast cancer. If someone feels that there is history of cancer especially Breast and /or ovarian should consults a medical personnel.
Causes Of Breast Cancer
While research is still evolving to ascertain the causes for Breast Cancer, it is generally caused due to the following factors:
1. Lifetsyle Issues:
A female’s body is governed by the interplay of estrogen and progesterone hormones. Estrogen promotes cell growth whereas Progesterone causes cell maturation and stabilization. In a woman’s life if estrogen exposure is more, it means more cell growth and cell multiplication, therefore more chances of mutation(changes which cause cancer) to occurleading to Breast cancer. Such situations occur with :
- Early Puberty
- Late or no Pregnancy
- Limited or No Breast Feeding
- Hormonal exposure in form of Hormonal replacement therapy or Hormones in any form; assisted reproduction methods
- Even increased stress and alcohol causes estrogen to rise in a woman’s body
- Obesity and lack of exercise also cause increased levels of estrogen
2. Environmental Factors :
Increased exposure to pollutants also contribute to rising Breast cancer in India.
- The carbon in the air pollution or when a woman smokes bind to the estrogen receptors in the body and breast. Today air pollution is on the rise and lot of women have started to smoke.
- The Pesticides and chemicals in our food and water also bind to these estrogen receptors and contribute to rise in Breast Cancer.
3. Hereditary factors :
There are certain genes like BRCA 1 and BRCA 2 which cause mainly Breast and Ovarian cancers run in the family. It means that if a woman harbour’s BRCA gene there is 80% chance that she will get Breast cancer in her lifetime and 40 % chance that she will get Ovarian cancer. There is a 50 % probability that the gene will be transferred to the next generation and can cause cancer.
The exact prevalence of these genes in Indian population is not yet known. In US, around 15% of Breast cancer is Hereditary. A lot more needs to be written about the Hereditary component of Breast Cancer which shall be followed in subsequent articles.
Screening & Early Detection
The only possible solution for the rising problem of Breast Cancer is early detection i.e. catching it at an early stage. At early stage with proper treatment we can expect 80 to 90% survival, 100% Breast preservation and high chances of de-escalation of adjuvant chemotherapy and radiation.
Breast Cancer screening in India is at very early stage, also we attribute it to Mammography whereas it forms just one small portion of Breast screening. According to American Cancer Society Guidelines, the standard screening process of mammography should start at the age of 45 followed by yearly intervals till the age of 55 and thereafter 2 yearly interval. In India as we know now, Breast Cancer women is a decade younger in comparison to western women, the disease peaks at 45 – 50 years. The Indian women have inherently higher breast density as compared to west. Both the facts suggest limited application of screening mammography in Indian settings. . For screening process to be effective it should start atleast 10 yrs. before the peak age of incidence. Advising Mammogram at the age of 35 is not at all effective
The manual breast screening methods in form of Self Breast Examination and Clinical Breast Examination are effective but sparingly used also sparingly used. Every woman should do a self Breast Examination. SBE is nothing but to be aware and conscious of the changes happening in one’s breast. If done regularly the woman can definitely detect Breast cancer if unfortunately it has to happen at a much early stage
How does Breast Cancer Present?
The Cancer presents as
- Lump in Breast
- Change in Nipple position in form of retraction or tethering
- Discharge from Nipple especially Bloody discharge
- Depression or scaring of Breast skin
- Redness or changes of Breast skin especially the Peu d orange form (skin looks and feel like orange peel)
- Fungating mass through the skin
- Mass or swelling in the armpit
Breast Lump Evaluation:
Clinical history and examination, which includes examination of Breast, axilla and neck to evaluate the primary tumor and nodal metastatic spread along with suspicion of distant sites. A clinical staging is also put forth.
The cause of the cancer is and need for genetic evaluation is ascertained.
- Routine blood and other standard evaluation
- Ultrasound and Mammogram (SONOMAMMOGRAM)
- According to the results further steps are planned. The report comes in BIRADS category.
- BI-RADS stands for Breast Imaging Reporting and Data System.
The following can be the result post Sonomammogram
- 0- incomplete
- 1-negative
- 2-benign findings
- 3-probably benign
- 4-suspicious abnormality
- 5-highly suspicious of malignancy
- 6-known biopsy with proven malignancy
Accordingly the following evaluation and treatment is done.
- BIRADS 1 & 2 are evaluated and treated as benign breast lumps
- BIRADS 4 and above are evaluated as malignant by doing a core needle biopsy/FNAB to confirm the malignancy
- BIRADS 3 the preference is to get a breast MRI
Breast MRI has basically three main uses
- Further evaluation of BIRADS 3 lesion, which suggests further whether to recommend a histological evaluation or keep the patient in follow up
- Evaluating Centricity or Focality of Breast Tumor: The MRI is a better investigation to make sure that their is no other focus of malignancy in the same breast both in the same quadrant as well as other quadrants and also in the other breast. This evaluation is very important to select the suitable patient for Breast Conservation surgical procedure
- Mammogram shows ACR C/D i.e. when the Breasts are dense which make them unsuitable for mammographic evaluation, Breast lumps or other pathologies occurring in these women will be evaluated by MRI
Followed by Clinical and radiological examination:
Histopathological evaluation is needed which is preferentially done by Core needle (Trucut) Biopsy to proof whether the lump is cancerous (Malignant) or not.
Core needle Biopsy is preferable or FNAC due
- Its better accuracy in terms of specificity i.e. false positivity
- It Provides tissue for IHC or Molecular analysis and categorization
Following histological confirmation, further diagnostic tests are prescribed according to clinical staging.
- If Clinically its an early stage disease i.e. lump size less than 5 cm with no palpable lymph nodes in axilla then tests for systemic evaluation shall be just Ultrasound abdomen and X ray of the chest.
- If clinically its an advanced stage disease i.e. a large size lump with or without changes in nipple and/or breast skin with palpable Lymph nodes in axilla and/or neck then systemic evaluation in form of CECT scan of chest and abdomen with bone scan with or without MRI Brain OR a whole body PET CT scan is required.
- MRI brain is more relevant in triple Negative Breast cancers.
Breast Cancer Treatment
Our Methodology of treating HER 2 Neu driven Breast Cancers
1. Preference to systemic therapy over upfront surgery
Even in early-stage breast cancer my preference is to go for systemic therapy over upfront surgery. This is not that surgical resection is not possible but to evaluate and understand the response to systemic treatment in primary as well as nodes. Patients in which response is good tend to do better and have lesser chances of recurrence. If upfront surgery is done, the chance of response assessment is lost forever.
We actually aim for complete response
2. Preference to Dual Anti Her 2 Neu agents
A dual blockade of ERBB2 pathway is preferrable in form of Traztuzumab + Pertuzumab with cytotoxic chemotherapy. The chances of complete response are better with dual blockade. Once the Neo Adjuvant treatment is over and complete response is reported in surgical specimen, and if resources are limited, we complete the rest of the Anti-Her 2 Neu treatment with single agent
3. Preventing Resistance to Anti Her 2 Neu therapy
- a. ERBB2 pathway leads to downstream upregulation PI3K- AKT – MTOR and RAS-RAF-MEK-ERK pathways. The response to ERBB2 blockade decreases if these pathways become independent of ERBB2 stimulation. PTEN downregulation also stimulates PI3K pathway independent of ERBB2
- b. Immune response plays important role as drugs used to block Her 2 Neu follow Antibody dependent cellular cytotoxicity and the cell debris then stimulate Antigen Presenting Cells which stimulate and direct NK cells
- c. Cancer stem cells stimulating through NF-KB pathway are remain behind after treatment and re-populate the cancer affected tissue leading to recurrence / residual disease.
Thus, we use Neutraceuticals specifically targeting PI3K; RAS-RAF and NF-KB pathways downregulating to decrease the chances of resisitance to anti Her 2 neu therapy
Also, we consider using Mistletoe and Thymosin Alpha to maintain the immune response and decrease the leukopenia to improve the efficacy of Anti Her2 Neu treatment.Robotic assistance in Breast surgery provides – visit here
- Seven degrees of Freedom
- Minimization of Tremor
- 3D – magnified view and resolution
- Improved Ergonomics
- Robotic Arms reach areas difficult to access like axilla and pelvis
If used properly, robotic assistance makes performing surgery easy, reduces complications with better aesthetics.
Breast Cancer Surgery today has two components one is resection or removal of tumor and the other is reconstructing the breast defect.
Breast Cancer Resection
Breast Cancer resection has evolved over the years. Modified Radical Mastectomy or Radical Mastectomy at present is indicated only in advanced cancers which do not respond to systemic therapy.
Oncoplastic Breast Preservation has now become the standard of care for Breast Cancer resection. Unless the skin and or the nipple is involved by the tumor or close; Skin sparing /Nipple sparing resections are being done as well as advocated. SSM/NSM are proven to have similar or even better oncological control as compared to more radical procedures like MRM with substantially better and gratifying aesthetic results.
Toesca etal from Milan for the past few years have started using Robotic assistance to perform Skin sparing / Nipple sparing procedures with Immediate Breast Reconstruction mainly through implants
There are substantial advantages of using Robotic Assistance: -
- Robotic arms provide better access at angles which is not possible with retractors in open methodology
- Enhanced Vision leads to precision dissection
- Incision placement is generally in skin creases like axillary(lateral) or inferior mammary creases given superior aesthetics than conventional Skin sparing procedures
- Skin flap Vascularity is better preserved by minimizing counter traction and incision planning
Breast Reconstruction:
Oncoplastic Breast Preservation defines reconstructing the Breast Defect either by Volume Displacement i.e., reshaping and realigning remaining breast tissue to form the Neo Breast or Volume Replacement i.e.; harvesting tissues from back, abdomen, thigh etc and bringing them to fill the breast defect which may be complete or partial mastectomy defect.
Latissimus tissue (LD flap) from lateral and posterior back area is the work horse flap used in Volume Replacement Oncoplasty. To harvest the LD flap via conventional methodology a long incision is placed in the back, the patient has to be repositioned and redraped majority of times.
Robotic Assistance provides:-
- Access to back(thorax) through axilla thus avoiding the incision and scar at the back, removing the need to reposition and redrape.
- The advantages robotic assistance in form of 3D – magnified view and resolution; improved ergonomics; better access to thorax provided by robotic arms helps in making the surgical procedure much simpler
Seiber et al suggested Robotic assistance decreases surgical time to half and also avoided the posterolateral thoracic i.e., back scar
Fourage et al confirmed Robot Assisted LD Flap to be a safe and effective procedure which offers precise dissection with minimal scarring.
We at CK Birla Hospitals are developing one of the first program for Robotic Breast Surgery in India. It will have both the components of Breast Cancer Surgery i.e., resection and reconstruction.
The Program Director is Dr Mandeep Singh Malhotra who is a Surgical & Molecular Oncologist with further specialization in Head Neck & Breast Oncology with more than 21 years of experience. He did is robotic training from UPENN, Pennsylvania USA.
He has one of the largest expeience Robot assisted Breast surgeries in India.
We proudly announce our Robotic Breast Surgery Program which shall make Breast surgery more precise, less morbid with highly improved aesthetics and faster recovery
Happy Patient with Dr Mandeep Singh Malhotra
